Das Endocannabinoid-System
Entdeckt in den frühen 90er Jahren durch Dr. Raphael Mechoulam, den Vater der medizinischen Cannabis-Forschung, bildet das Endocannabionid-System die Basis zum Verständnis, wie Cannabis auf unseren Organismus wirkt. Das Endocannabinoid-System ist ein bestimmender Regulator verschiedener Körperfunktionen.
Es gibt kaum einen funktionellen Prozess, der nicht bis zu einem gewissen Grad davon beeinflusst wird.
Trotz der herausragenden Bedeutung des Endocannabinoid-Systems als wesentlicher Regulationsmechanismus in der Biochemie und Physiologie des Körpers sind die Kenntnisse über dieses System nach wie vor recht begrenzt, insbesondere unter deutschen Ärzten.
Gerade hier sehen wir bei der LGP einen hohen Bedarf an Aufklärung sowie Ausbildung.
Unsere ausgebildeten Ärzte werden Sie im Erstgespräch, welches Sie ganz bequem von zu Hause aus digital durchführen können, nicht nur über Cannabis als Medizin, sondern auch über das ECS und dessen Aufgaben aufklären.
Aufbau des ECS
Was sind Cannabinoide?
Phytocannabinoide gehören zur Klasse der Cannabinoide. Diese chemischen Verbindungen kommen in der Cannabis-Pflanze vor. Sie binden an die Cannabinoid-Rezeptoren und nehmen so Einfluss auf die Freisetzung von Botenstoffen im Gehirn. Die zwei bekanntesten Phytocannabinoide sind THC (Tetrahydrocannabinol) und CBD (Cannabidiol).
Endocannabinoide (körpereigene Cannabinoide) gehören ebenfalls zur Klasse der Cannabinoide. Diese werden von unserem Körper hergestellt und imitieren die Wirkungsweise der Phytocannabinoide.
Die zwei primären Endocannabinoide sind AEA (Arachdionylethanolamin), das nach dem Sanskrit-Wort für “Glückseligkeit“ auch Anandamid genannt wird und 2-AG (2-Arachidonylglycerol).
Die Rolle der Endocannabinoide besteht darin, die Homöostase (Gleichgewicht) zu erhalten. Sie sorgen dafür, dass unsere Zellen effektiv, aber nicht übermäßig miteinander kommunizieren.
Cannabinoid-Rezeptoren
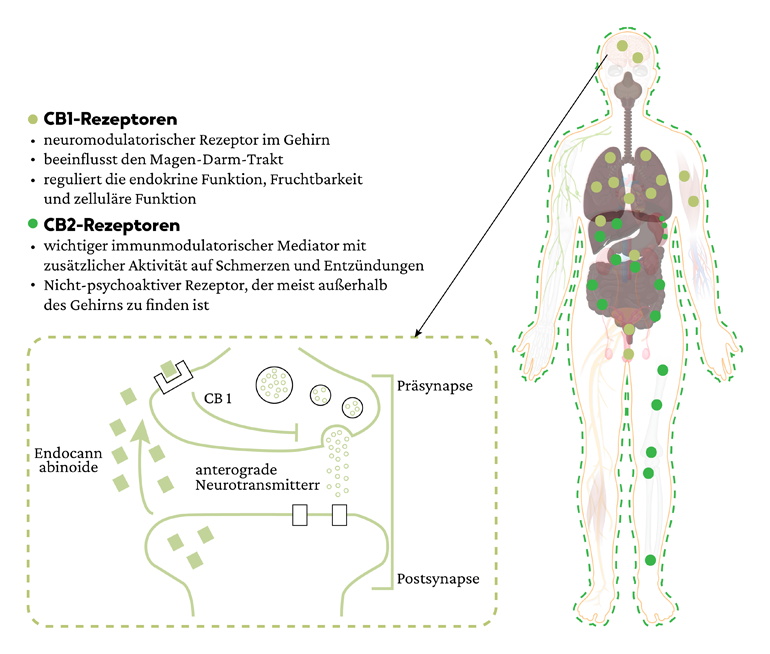
Im ECS gibt es zwei Hauptrezeptoren – CB1 und CB2.
Einen Rezeptor kann man sich als Schloss vorstellen zu dem ein entsprechender Stoff wie ein Schlüssel (wenn er die richtige Struktur hat) passt. Gelangt der Schlüssel in das Schloss laufen weitere chemische Vorgänge im Zellinneren ab.
CB1-Rezeptoren überwiegen im zentralen Nervensystem, wo sie eine übermäßige Übertragung von Botenstoffen eindämmen. Sobald Nervenzellen eine übermäßige Menge an chemischen Botenstoffen freisetzen, wirken die Endocannabinoide quasi als Bremse, damit eine Balance sichergestellt werden kann.
CB2-Rezeptoren sind im gesamten Körper verteilt, vor allem in den Zellen des Immunsystems und des Magen-Darm-Trakts.
Endocannabinoide aktivieren CB2-Rezeptoren, die sich an den Zellmembranen befinden. Sobald die CB2-Rezeptoren aktiviert sind, lösen sie zahlreiche immunverändernde Wirkungen aus, die von der Art der Zelle und ihrer Umgebung abhängen. Die Aktivierung von CB2-Rezeptoren führt zu einer Reduktion der Freisetzung von entzündlichen Botenstoffen (Zytokinen). Dies hat positive klinische Auswirkungen.
Enzyme
Das ECS steht weitgehend unter enzymatischer Kontrolle. Der Gehalt an Endocannabinoiden wird durch das Gleichgewicht zwischen der Herstellung von Enzymen und deren Abbau bestimmt. Sie sorgen dafür, dass die Endocannabinoide dann verwendet werden, wenn sie gebraucht werden.
Referenzen
Referenzen:
1. Light, M. K., A. Orens, B. Lewandowski, and T. P. Market size and demand for marijuana in Colorado. (2014).
2. Ilgen, M. A. et al. Characteristics of adults seeking medical marijuana certification. Drug Alcohol Depend. 132, 654–659 (2013).
3. Boehnke, K. F., Litinas, E. & Clauw, D. J. Medical Cannabis Use Is Associated with Decreased Opiate Medication Use in a Retrospective Cross-Sectional Survey of Patients with Chronic Pain. J. Pain 17, 739–744 (2016).
4. Whiting, P. F. et al. Cannabinoids for medical use: A systematic review and meta-analysis. JAMA - J. Am. Med. Assoc. 313, 2456–2473 (2015).
5. Ware, M. A. et al. Smoked cannabis for chronic neuropathic pain: A randomized controlled trial. Cmaj 182, (2010).
6. Mechtler, L. L., Gengo, F. M. & Bargnes, V. H. Cannabis and Migraine: It’s Complicated. Curr. Pain Headache Rep. 25, 1–13 (2021).
7. Rhyne, D. N., Anderson, S. L., Gedde, M. & Borgelt, L. M. Effects of Medical Marijuana on Migraine Headache Frequency in an Adult Population. Pharmacotherapy 36, 505–510 (2016).
8. Russo, E. Cannabis for migraine treatment: The once and future prescription? An historical and scientific review. Pain 76, 3–8 (1998).
9. Cuttler, C., Spradlin, A., Cleveland, M. J. & Craft, R. M. Short- and Long-Term Effects of Cannabis on Headache and Migraine. J. Pain 21, 722–730 (2020).
10. Baron, E. P. Medicinal Properties of Cannabinoids, Terpenes, and Flavonoids in Cannabis, and Benefits in Migraine, Headache, and Pain: An Update on Current Evidence and Cannabis Science. Headache 58, 1139–1186 (2018).
11. Serpell, M. et al. A double-blind, randomized, placebo-controlled, parallel group study of THC/CBD spray in peripheral neuropathic pain treatment. Eur. J. Pain (United Kingdom) 18, 999–1012 (2014).
12. Hoch, E. et al. How effective and safe is medical cannabis as a treatment of mental disorders? A systematic review. Eur. Arch. Psychiatry Clin. Neurosci. 269, 87–105 (2019).
13. Bachhuber, M., Arnsten, J. H. & Wurm, G. Use of Cannabis to Relieve Pain and Promote Sleep by Customers at an Adult Use Dispensary. J. Psychoactive Drugs 51, 400–404 (2019).
14. Shannon, S., Lewis, N., Lee, H. & Hughes, S. Cannabidiol in Anxiety and Sleep: A Large Case Series. Perm. J. 23, 18–041 (2019).
15. Piper, B. J. et al. Substitution of medical cannabis for pharmaceutical agents for pain, anxiety, and sleep. J. Psychopharmacol. 31, 569–575 (2017).
16. Corroon, J. M., Mischley, L. K. & Sexton, M. Cannabis as a substitute for prescription drugs - A cross-sectional study. J. Pain Res. 10, 989–998 (2017).
17. Duran, M. et al. Preliminary efficacy and safety of an oromucosal standardized cannabis extract in chemotherapy-induced nausea and vomiting. Br. J. Clin. Pharmacol. 70, 656–663 (2010).
18. Hernandez, S. L., Sheyner, I., Stover, K. T. & Stewart, J. T. Dronabinol Treatment of Refractory Nausea and Vomiting Related to Peritoneal Carcinomatosis. Am. J. Hosp. Palliat. Med. 32, 5–7 (2015).
19. Merriman, A. R. & Oliak, D. A. Use of medical marijuana for treatment of severe intractable nausea after laparoscopic Roux-en-Y gastric bypass surgery. Surg. Obes. Relat. Dis. 4, 550–551 (2008).
20. Westfall, R. E., Janssen, P. A., Lucas, P. & Capler, R. Reprint of: Survey of medicinal cannabis use among childbearing women: Patterns of its use in pregnancy and retroactive self-assessment of its efficacy against ‘morning sickness’. Complement. Ther. Clin. Pract. 15, 242–246 (2009).
21. Gonzalez-Rosales, F. & Walsh, D. Intractable nausea and vomiting due to gastrointestinal mucosal metastases relieved by tetrahydrocannabinol (Dronabinol). J. Pain Symptom Manage. 14, 311–314 (1997).
22. Green, S., Nathwani, D., Goldberg, D. & Kennedy, D. Nabilone as effective therapy for intractable nausea and vomiting in AIDS [letter]. Br. J. Clin. Pharmacol. 28, 494–495 (1989).
23. Dejesus, E., Rodwick, B. M., Bowers, D., Cohen, C. J. & Pearce, D. Use of dronabinol improves appetite and reverses weight loss in HIV/AIDS-infected patients. J. Int. Assoc. Physicians AIDS Care 6, 95–100 (2007).
24. Zutt, M., Hänßle, H., Emmert, S., Neumann, C. & Kretschmer, L. Dronabinol zur supportiven Therapie metastasierter maligner Melanome mit Lebermetastasen. Hautarzt 57, 423–427 (2006).
25. Volicer, L., Stelly, M., Morris, J., McLaughlin, J. & Volicer, B. J. Effects of dronabinol on anorexia and disturbed behavior in patients with Alzheimer’s disease. Int. J. Geriatr. Psychiatry 12, 913–919 (1997).
26. Cooper, R. E. et al. Cannabinoids in attention-deficit/hyperactivity disorder: a randomised-controlled trial. Eur. Neuropsychopharmacol. 26, S130 (2016).
27. Aharonovich, E. et al. Concurrent cannabis use during treatment for comorbid ADHD and cocaine dependence: Effects on outcome. Am. J. Drug Alcohol Abuse 32, 629–635 (2006).
28. Hupli, A. M. M. Medical Cannabis for Adult Attention Deficit Hyperactivity Disorder: Sociological Patient Case Report of Cannabinoid Therapeutics in Finland. Med. Cannabis Cannabinoids 1, 112–118 (2019).
29. Prentiss, D., Power, R., Balmas, G., Tzuang, G. & Israelski, D. M. Patterns of Marijuana Use among Patients with HIV/AIDS Followed in a Public Health Care Setting. J. Acquir. Immune Defic. Syndr. 35, 38–45 (2004).
30. Consroe, P. M. R. R. J. T. W. P. R. The Perceived Effects of Smoked Cannabis on Patients with Multiple Sclerosis. Eur. Neurol. (1997) doi:10.1159/000112901.
31. Linares, I. M. P. et al. No acute effects of Cannabidiol on the sleep-wake cycle of healthy subjects: A randomized, double-blind, placebo-controlled, crossover study. Front. Pharmacol. 9, 1–8 (2018).
32. Bonaccorso, S., Ricciardi, A., Zangani, C., Chiappini, S. & Schifano, F. Cannabidiol (CBD) use in psychiatric disorders: A systematic review. Neurotoxicology 74, 282–298 (2019).
33. Neubauer, D., Perkovic Benedik, M. & Osredkar, D. Cannabidiol for treatment of refractory childhood epilepsies: Experience from a single tertiary epilepsy center in Slovenia. Epilepsy Behav. 81, 79–85 (2018).
34. Devinsky, O. et al. Cannabidiol in patients with treatment-resistant epilepsy: an open-label interventional trial. Lancet Neurol. 15, 270–278 (2016).
35. Szaflarski, J. P. et al. Long-term safety and treatment effects of cannabidiol in children and adults with treatment-resistant epilepsies: Expanded access program results. Epilepsia 59, 1540–1548 (2018).
36. Hausman-Kedem, M., Menascu, S. & Kramer, U. Efficacy of CBD-enriched medical cannabis for treatment of refractory epilepsy in children and adolescents – An observational, longitudinal study. Brain Dev. 40, 544–551 (2018).
